Table of Content
Early identification of this diagnosis, as well as the sub-type of priapism, allows for rapid initiation of indicated treatments. Thus, collaboration between emergency medicine physicians and urologic specialists is imperative to the provision of appropriate, timely care. Early penile prosthesis placement in management of acute ischemic priapism. First-lineThe treatment of each acute episode is similar to that of low-flow priapism.Drug therapyHormonal therapies and/or antiandrogens or phosphodiesterase type 5 inhibitors, depending on the patient’s medical profile. Sickle cell patients – This group of patients may require a specific regime of therapy to treatment their sickle cell disease, including oxygenation, hydration, alkalinization, analgesia and exchange transfusion. When an erection lasts for too long, this oxygen-poor blood can begin to damage or destroy tissues in the penis.
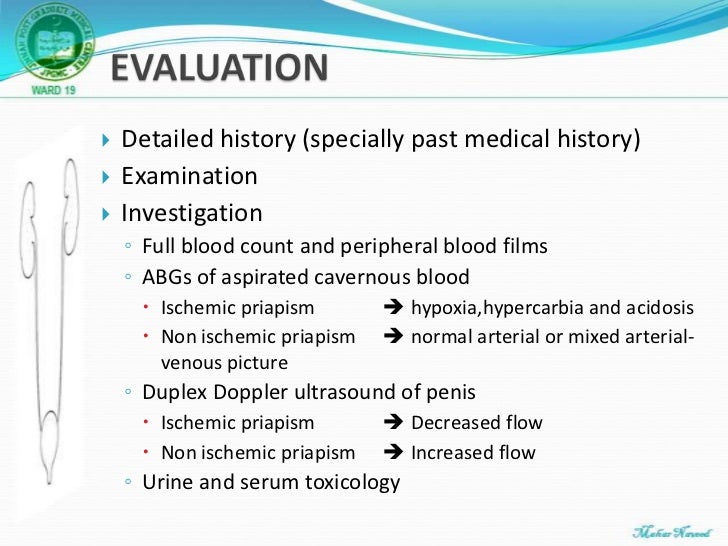
Penile duplex Doppler ultrasonography is not the primary way to diagnose priapism. While radiologic imaging studies have demonstrated utility in the evaluation and management of priapism, this is largely outside of the acute phase of presentation. As such, imaging studies should not be incorporated into the acute evaluation and management of priapism in the emergency department by non-urologist specialists.
What is priapism?
Likewise, if the prospects of functional recovery are dramatically low, clinicians may wish to weigh and consider the potential detriment of distal shunting for patients who may elect subsequent implant placement. Potential non-erectile complications of distal shunting and tunneling procedures include urethral injury, cavernositis, persistence of fistula, infection, and penile skin necrosis. The initial presentation of priapism often happens acutely and in the setting of an emergency department.
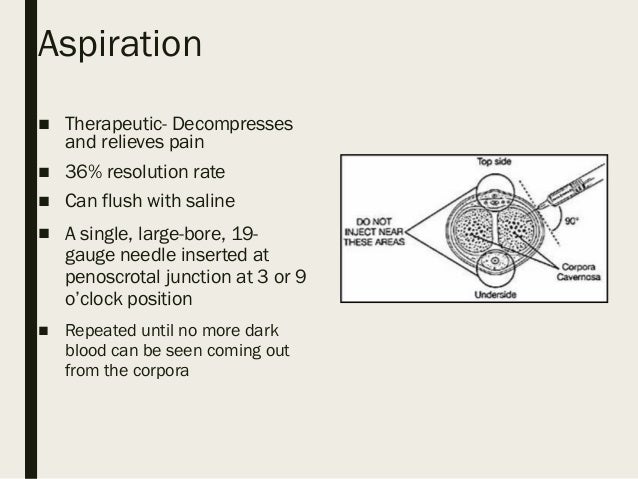
As such, there are likely no surgeons who have extensive experience in this area, and broader training and education on methods of optimizing outcomes are therefore not possible. Additionally, the extent and rate of complications from proximal shunting is understudied and could potentially lead to significant comorbidities such as urethrocutaneous fistulae, urethral strictures, or other similar issues. From a practical standpoint, such limited data would typically relegate a procedure to experimental status. Additionally, some of the described procedures require distinct skillsets outside of a general urologist’s training, including performing vascular anastomoses to the saphenous or dorsal penile vein. Corporal aspiration refers to the intracavernosal placement of a needle followed by withdrawal of corporal blood. Irrigation indicates subsequent instillation of fluid into the corpora.
Guideline Statements
However, each of these conditions is likely distinct from recurrent ischemic priapism given the lack of underlying ischemia and without the need for emergent intervention. Similarly, very limited data exist on management strategies of these conditions, and their existence and optimal treatments remain investigational at the present time. Further research, including multicenter registries are merited given the relative low prevalence of these conditions and significant heterogeneity in diagnosis and treatment.

In cases where the fistula is unchanged and/or where patient bother is significant, intervention may be considered. All diagnosed NIP patients should undergo a period of at-home observation to determine if the fistula will close spontaneously resulting in penile detumescence. It is worth noting that many men with NIP will have observed themselves at home for extended periods of time before clinical presentation, and therefore, may have already fulfilled their period of observation. Clinicians should counsel patients that non-ischemic priapism is not an emergency condition and should offer patients an initial period of observation.
What are the causes and risk factors of priapism?
The data to evaluate the utility of tunneling is very limited and of low quality. There are no RCTs or comparative studies, and observational studies preclude unbiased comparisons between distal shunts with and without tunneling. The genitalia, perineum, and abdomen should be carefully examined. In patients with priapism, the corpora cavernosa are typically affected while the corpus spongiosum and the glans penis are not. Further, the corpora cavernosa in acute ischemic priapism patients are often fully rigid and tender, while men with NIP exhibit partial corporal tumescence .
Once finalized, the guideline was submitted for approval to the AUA PGC, Science and Quality Council, Board of Directors, and the governing bodies of SMSNA. Studies rated “high risk of bias” have significant flaws that may invalidate the results. They have a serious or “fatal” flaw in design, analysis, or reporting; large amounts of missing information; discrepancies in reporting; or serious problems in the delivery of the intervention. The results of high risk of bias studies could be as likely to reflect flaws in study design and conduct as true differences between compared interventions.
Priapism treatment
The major neurotransmitter that controls erection is nitric oxide, which is secreted by the endothelium that lines the corpora cavernosa . Diseases Treatments Dictionary Complete solution for all diseases && disorders treatments. To know any Diseases that which may it causes, symptoms on your body, and how can prevent from them, what to do on first aid, Definition’s, Diagnosis and Test, Risk Factors, specific treatments. In addition to the aspiration of the penis, a medication like epinephrine, an alpha agonist, can be administered to encourage vascular contraction to deflate the erection.
Presence of normal to high velocities in the cavernous arteries should be expected in the setting of NIP. Ultrasonography should be performed in the lithotomy or frogleg position, scanning the perineum first and then along the entire shaft of the penis. Ultrasonography is of particular benefit in a patient with NIP being considered for fistula embolization. This allows for communication between the urologist and radiologist prior to intervention regarding fistula location, size, and eventual choice of vascular access.
Whether you see a urologist or an emergency room provider, the initial aim of an evaluation to resolve an enduring erection is to distinguish which type of priapism is at play. Patients struggling with recurrent priapism sometimes also suffer, or have suffered, from ischemic priapism. After approximately four hours, when the environment becomes ischemic enough, patients perceive pain, he said. The ischemic variety tends to be idiopathic, or without a known cause, and occurs most often. A case of ischemic priapism must be managed quickly given the severe consequences of waiting, Akakpo said.
This can help your doctor diagnose blood disorders, cancers, and sickle cell anemia. The Panel recommends that the clinician perform repeat embolization in patients who are refractory to embolization. This should be done in the context of shared decision making after the patient is aware of the surgical options. Furthermore, while fistula ligation has historically been performed, it is an outdated procedure and there is inadequate evidence to quantify the benefit of the procedure. The Panel recommends this approach, as it is likely to be more effective and safer than an attempt at surgical ligaton, given the lack of experience in the latter approach for most urologists and the poor data supporting ligation. PDUS may be performed in a non-urgent fashion in a patient with NIP to help with screening for anatomical abnormalities and identification of cavernous artery fistula or pseudoaneurysm location and size.
"They're completely different," said William Akakpo, M.D., a urologic surgeon at Paris Urology and Andrology Center and one of the authors of the 2018 article. "You have the ischemic priapism—we call it 'low-flow' priapism—an emergency situation demanding urgent care to avoid definitive erectile dysfunction." Identifying a role of sexual health counselor in patients with acute ischemic priapism undergoing surgery and how this affects short- and long-term mental health.
We did not exclude studies rated high risk of bias a priori but considered such studies to have low reliability. The objective of the current Guideline is to provide a practical guide that is directive in cases where evidence is more abundant while remaining flexible to allow for clinician judgment. As such, the Guideline does not establish a fixed set of rules for the treatment of priapism.
Specifically, the role of imaging (e.g., ultrasound, CT, MRI) is clarified during the initial diagnosis as well as post-treatment, such as with men exhibiting persistent pain or perceived rigidity post distal shunting. If the penis has been erect for fewer than 4 hours, decongestant medications to decrease blood flow to the penis can be effective at reducing the erection. If the erection has lasted for 4-6 hours, medication is usually effective. Medications, including erectile dysfunction drugs, blood thinners, antidepressants, and some blood pressure drugs can cause priapism.









No comments:
Post a Comment